
The Canadian Federation of Medical Students
Mental Health Wellness
Medical training is intellectually demanding and emotionally complex. Long hours, high expectations, exposure to suffering, and performance pressure can challenge even the most resilient students. This guide focuses on building insight, resilience, recovery, and accessible support strategies.Mental Health
Medical students and physicians experience higher rates of burnout, depression, anxiety, and psychological distress compared to age-matched peers. Contributing factors include:
- Perfectionism and high self-expectations
- Academic and clinical workload
- Sleep disruption
- Exposure to trauma and suffering
- Mistreatment or hierarchical pressures
- Transitions (pre-clerkship → clerkship → CaRMS)
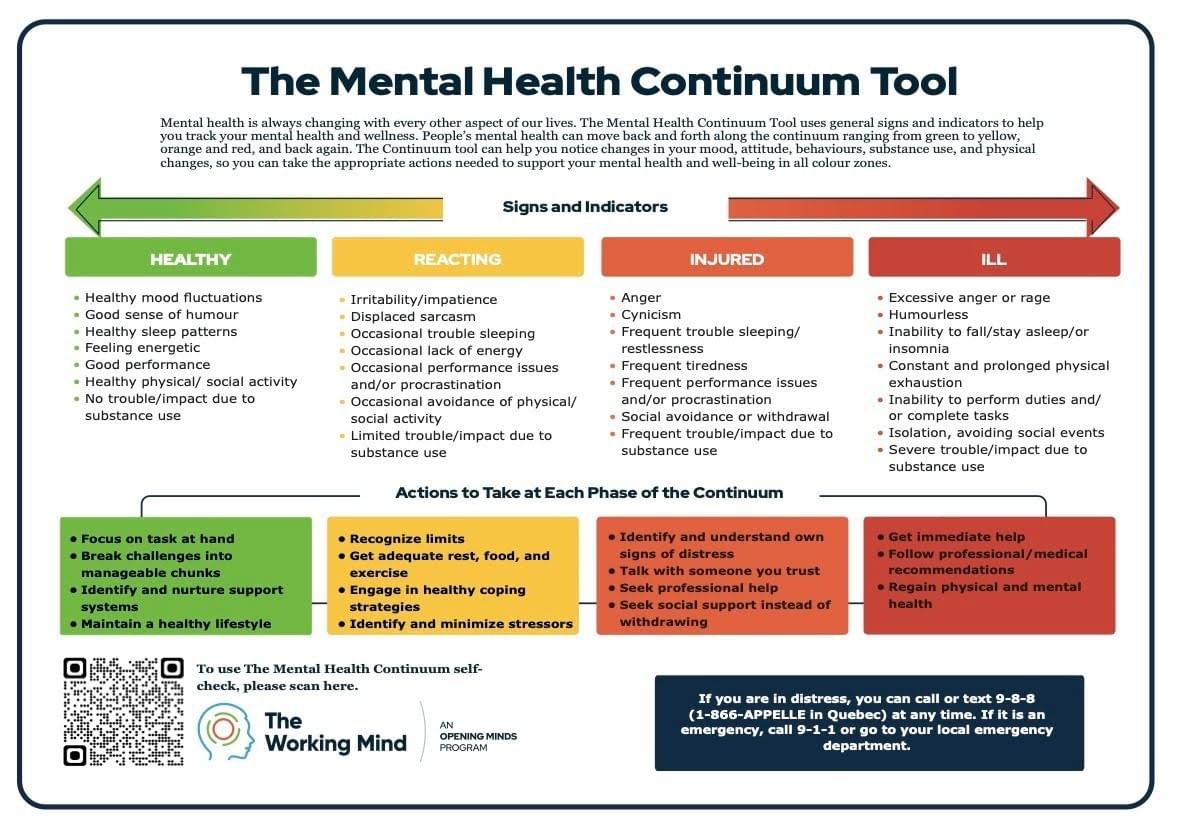
The Mental Health Continuum is a quick and easy tool that can be used to monitor mental wellness and burnout - your results may surprise you.
Burnout is commonly described as:
- Emotional exhaustion
- Depersonalization or cynicism
- Reduced sense of accomplishment
Importantly, distress during training is common, but it is not inevitable, and it is not a personal failure. There is more on burnout and compassion fatigue below.
Clerkship additionally introduces repeated exposure to suffering, death, and moral complexity. This can result in:
- Emotional blunting
- Guilt about “not feeling enough”
- Carrying patient stories home
- Self-doubt after difficult encounters or feedback/criticism
Medical students may benefit from:
- Self-care strategies, such as rest, mindfulness and movement
- Debriefing with peers, residents, and/or staff
- Asking mentors how they process difficult cases
- Recognizing emotional reactions as human, not weakness
Mistreatment and Emotional Safety
Mistreatment and emotional safety is a commonly reported challenge for medical students.
Hierarchical systems can contribute towards:
- Public criticism
- Dismissive feedback
- Discrimination
- Intimidation
Medical students may benefit from:
- Knowing reporting pathways
- Accessing ombudsperson or learner affairs offices
- Connecting with student wellness representatives
- Peer discussion spaces
Psychological safety improves learning and performance.
National Voice, Advocacy, and Peer Stories
Peer storytelling reduces isolation and normalizes help-seeking. Engaging in advocacy can also lead to empowerment and positive change. Organizations like the CFMS leads initiatives like national-level advocacy and peer collaboration, as featured on their socials. Examples of this include:
- Peer-submitted stories (burnout, compassion fatigue, recovery, mistreatment experiences)
- Reflections on growth and resilience
- “What I wish I knew in first year” narratives
- Clerkship transition experiences
Mindfulness
Time-efficient mindfulness practices can contribute towards realistic mental health maintenance strategies.
- Mindfulness does not require a 30-minute meditation session
- For medical trainees, micro-practices are often more sustainable and can be self-directed
- Apps like Headspace have mental health and mindfulness resources and programming
- The Mindfulness Council of Canada has a database of formalized local programs
Rest
Rest is a valuable tool. In medicine, rest is often framed as optional. In reality, rest improves:
- Memory consolidation
- Clinical reasoning
- Emotional regulation
- Empathy
- Decision-making
Rest strategies:
- Protect 1–2 “non-negotiable” rest windows weekly
- Keep a wind-down routine (even 10 minutes)
- Limit caffeine late in the day
- Avoid doom-scrolling as default decompression
- Reduce or eliminate screen time before sleep
- Consider Heart and Stroke Foundation of Canada’s recommendations for improved sleep hygiene
Rest is not indulgent — it is protective.
Movement
Exercise will be covered extensively in the “Physical Wellness” section, but it is worth mentioning as a valuable contributor towards mental health and well-being. Even when time is limited, finding opportunities to take short walks or stretch breaks can be refreshing and grounding during long on-call shifts.
Journaling and Reflection
Reflection improves insight, emotional processing, and resilience.
Quick journal prompts:
- What challenged me today?
- What did I handle better than I thought?
- What did I learn about myself?
- What would I say to a friend in my position?
Gratitude tracking:
Instead of “3 perfect things,” try:
- One thing that felt steady
- One person who helped
- One small win
Consistency matters more than depth.
When to Seek Help
It is important to acknowledge when you need help. Mental health decline can be gradual and insidious. Listen to your peers and loved ones if they express concerns regarding your mental health, and engage with tools like the Mental Health Continuum to monitor your own well-being.
If you find yourself sliding towards the orange and red - seek help. This can involve reaching out to your school’s learner wellness office to discuss resources, and/or reaching out to a professional such as a clinical counsellor. Early intervention can be preventative.
If in distress, seek immediate help. On-demand resources exist in the form of local mental health crisis lines, the 988 national suicide crisis line, 911 emergency resources, and the emergency department.
Keep an eye on your peers, and look out for each other on this journey. Checking in on peer mental health and well-being can help reduce stigma and open up a forum for discussion.
On-Call Mental Health Kit
A Practical Reset Guide for Medical Students
Prepared by the Canadian Federation of Medical Students
On-call shifts are demanding. On-call work is cognitively intense and emotionally unpredictable. This guide is not about being perfectly regulated — it is about staying steady enough to function well and recover afterward.
1. Before the Shift
Protect your baseline.
Quick 30-second check-in:
- Have I eaten?
- Do I have water?
- What kind of shift is this likely to be? What should I mentally prepare for?
Set one intention:
- “Steady, not perfect.”
- “One patient at a time.”
- “Ask for help early.”
- “I am a student, I am not expected to know everything.”
Pack:
- Water bottle
- 1–2 balanced protein and carb meals/snacks
- Small comfort item (tea bag, gum, photo, playlist)
2. During the Shift
Micro-Regulation Tools (1–2 minutes)
Breathing reset
- Box breathing: Inhale 4 seconds – hold 4 seconds – exhale 6 seconds
- Repeat 4 times before presentations or after pages
Grounding (“name 3”)
- 3 things you see
- 3 things you feel physically
- 3 things you hear
Cognitive reframe
- Instead of: “I’m behind. I’m terrible at this.”
- Try: “This is a heavy shift. I’m learning in real time.”
3. Emotional First Aid
Common on-call reactions:
- Self-doubt after feedback
- Emotional blunting
- Irritability or shutdown
- Guilt about not knowing enough
Stabilization techniques:
- Step outside for 2 minutes
- Splash cool water on your face
- Text a trusted peer
- Write one processing note to revisit later
You do not need to process everything mid-shift — just contain it.
4. Protect Your Energy
- Eat every 3–4 hours (even something small)
- Alternate caffeine with water
- Sit when charting if possible
- Cluster tasks to reduce mental switching
Fatigue amplifies negative thinking. Fueling supports cognition.
5. After the Shift
Close the loop. Before leaving, reflect on:
- One thing that went well
- One thing I learned
- One thing I am leaving here
Create a transition ritual:
- Change shoes
- Play one consistent “end of shift” song
- Take 5 slow breaths before driving
- Shower immediately on arriving home
Signal to your brain: the shift is over.
6. Know When to Reach Out
Seek support if you notice:
- Persistent dread before shifts
- Panic symptoms
- Sleep that does not recover post-call
- Intrusive replaying of cases
- Thoughts of self-harm
Consider contacting:
- Your school’s learner wellness office
- Confidential counseling services
- Provincial physician health programs
- Local crisis resources
Early support is protective — not a sign of weakness.
REMINDER
You are learning in a high-stakes system.
You will not know everything.
You are allowed to be new.
Steady > Perfect
Burnout Literature Review
Prevalence in Canadian Medical Students & Physicians
Burnout — typically defined as a syndrome encompassing emotional exhaustion, depersonalization, and reduced personal accomplishment — is consistently elevated across the medical training continuum. It has been measured using widely used tools such as the Maslach Burnout Inventory (MBI) in multiple Canadian studies.
Medical Students
Research indicates that burnout is highly prevalent among medical students in Canada. In a meta-analytic review that included Canadian cohorts, the pooled prevalence of burnout in medical students was approximately 27.6% in Canada, with overall estimates globally around 37% when measured using instruments such as the MBI and related inventories (e.g. emotional exhaustion, depersonalization, and reduced personal accomplishment) (Almutairi et al., 2022). A Canadian cross-sectional survey found that 37% of Canadian medical students met criteria for burnout, with clinically relevant levels of emotional exhaustion and other psychological distress noted (Lewis & Bhugra, 2022).
Residents
Burnout prevalence among Canadian residents is likewise high. A national survey of Royal College emergency medicine residents reported that 62% met established burnout criteria on the MBI, highlighting widespread symptoms even early in postgraduate training (Liu et al., 2020). Additional multi-specialty research has reported prevalence estimates in Canadian residents around 58%–69%, with emotional exhaustion and depersonalization particularly elevated, and associations with excessive work hours and work-life imbalance (Shalaby et al., 2023; L. Shalaby et al., 2023).
Physicians
Among practising Canadian physicians, burnout continues to be a significant concern. Surveys during the COVID-19 era found that ~60% of Canadian emergency physicians reported high burnout, including elevated emotional exhaustion and/or depersonalization (Chan et al., 2021). National physician health surveys indicate that over half of Canadian physicians report burnout symptoms, with higher rates observed among early-career clinicians (less than 20 years in practice) and across multiple specialties (Canadian Medical Association, 2021). A national study focused on Canadian physiatrists found that 42% met burnout criteria in a representative sample, with younger age and emotion-regulation difficulties linked to higher risk (Simpson et al., 2025).
References
Almutairi, H., Alsubaiei, A., Abduljawad, S., Alshatti, A., Fekih-Romdhane, F., Husni, M., … Jahrami, H. (2022). Prevalence of burnout in medical students: A systematic review and meta-analysis. International Journal of Social Psychiatry.
Canadian Medical Association. (2021). 2021 National Physician Health Survey: Burnout and workload reductions. Canadian Medical Association.
Chan, T., et al. (2021). Canadian emergency medicine physician burnout during the COVID-19 pandemic. Canadian Journal of Emergency Medicine.
Lewis, T., & Bhugra, D. (2022). Wellbeing and mental health amongst medical students in Canada.
Liu, R., Van Aarsen, K., Sedran, R., & Lim, R. (2020). A national survey of burnout amongst Canadian Royal College emergency medicine residents. Canadian Medical Education Journal, 11(5), 1–9. https://doi.org/10.36834/cmej.68602
Shalaby, L., Oluwasina, F., El Gindi, H., Eboreime, E., Nwachukwu, I., Hrabok, M., … Agyapong, V. (2023). Burnout among physicians: Prevalence and predictors among resident doctors in Canada. Abstract presented in European Psychiatry.
Simpson, R., Cohen, E., Kiss, A., Wasilewski, M., Hitzig, S., … Bayley, M. (2025). Burnout in Canadian physiatrists: A national cross-sectional survey. American Journal of Physical Medicine & Rehabilitation.
Compassion Fatigue in Medical Training
A brief evidence summary for medical students.
What Is Compassion Fatigue?
Compassion fatigue is often described as the emotional and physical exhaustion that can occur from repeated exposure to others’ suffering. It is closely related to secondary traumatic stress and shares features with burnout, but is conceptually distinct (Figley, 1995; Stamm, 2010).
Whereas burnout is primarily associated with chronic workplace stress and systemic overload, compassion fatigue is more directly linked to exposure to patients’ trauma, grief, and distress (Figley, 2002).
Core features may include:
- Emotional exhaustion
- Reduced capacity for empathy
- Irritability or emotional numbing
- Intrusive thoughts related to patient care
- Avoidance of emotionally charged cases
Compassion Fatigue in Medical Students & Physicians
Although compassion fatigue has been more extensively studied in nursing and trauma professionals, research increasingly demonstrates its relevance to physicians and trainees.
A systematic review of physicians found substantial rates of burnout and secondary traumatic stress across specialties, particularly in high-acuity environments (Rotenstein et al., 2018). While the review focused primarily on burnout and depression, many included studies identified emotional exhaustion linked to patient suffering exposure.
Emergency medicine physicians and residents report high levels of emotional exhaustion and depersonalization, particularly during periods of crisis (e.g. pandemics), suggesting vulnerability to compassion fatigue processes (Chan et al., 2021).
Among medical trainees, repeated exposure to death, critical illness, ethical tension, and high-stakes uncertainty during clerkship has been associated with emotional blunting and reduced empathy over time (Neumann et al., 2011).
The risk of compassion fatigue increases with:
- High patient acuity or trauma exposure
- Repeated exposure to death or moral distress
- Lack of debriefing opportunities
- Sleep deprivation
- Perfectionism and high self-expectations
- Limited psychological safety in clinical environments
Clerkship can be a particularly vulnerable period due to emotional exposure combined with low perceived control.
Distinguishing Burnout vs. Compassion Fatigue
Burnout
Exposure to chronic workplace stress
Gradual onset
Cynicism towards work
Workload/system driven
Compassion Fatigue
Exposure to patient suffering
Can have more acute emotional shifts
Emotional numbing toward patients
Trauma/empathy driven
They frequently co-occur but may require different prevention approaches.
Protective Factors
Evidence suggests protective factors include:
- Structured debriefing after difficult cases
- Peer support and normalization
- Reflective practice
- Emotion regulation skills
- Meaning-making and values alignment
- Mentorship relationships
Empathy can be preserved when trainees are supported rather than left to process difficult cases alone (West et al., 2016).
Why This Matters
Compassion fatigue is not a sign of weakness or lack of caring. It often occurs because someone cares deeply. When unrecognized, it may contribute to:
- Reduced well-being
- Depersonalization
- Increased medical errors
- Career dissatisfaction
Early recognition and supportive environments are key.
References
Chan, T. M., et al. (2021). Burnout and wellness in Canadian emergency physicians during the COVID-19 pandemic. Canadian Journal of Emergency Medicine, 23(4), 551–560.
Figley, C. R. (1995). Compassion fatigue: Coping with secondary traumatic stress disorder in those who treat the traumatized. Brunner/Mazel.
Figley, C. R. (2002). Compassion fatigue: Psychotherapists’ chronic lack of self-care. Journal of Clinical Psychology, 58(11), 1433–1441.
Neumann, M., Edelhäuser, F., Tauschel, D., et al. (2011). Empathy decline and its reasons: A systematic review of studies with medical students and residents. Academic Medicine, 86(8), 996–1009.
Rotenstein, L. S., Torre, M., Ramos, M. A., et al. (2018). Prevalence of burnout among physicians: A systematic review. JAMA, 320(11), 1131–1150.
Stamm, B. H. (2010). The concise ProQOL manual. ProQOL.org.
West, C. P., Dyrbye, L. N., Erwin, P. J., & Shanafelt, T. D. (2016). Interventions to prevent and reduce physician burnout: A systematic review and meta-analysis. The Lancet, 388(10057), 2272–2281.
